

Pleuroscopy by Flexible Thoracoscope
Pleuroscopy, also known as medical thoracoscopy, is a minimally invasive procedure that allows direct visualization of the pleural space—the area between the lungs and the chest wall. Using a flexible thoracoscope, this technique helps diagnose unexplained pleural effusions and take biopsy samples with minimal discomfort.
Dr. Manoj Kumar Goel, a renowned pulmonologist in Delhi, offers expert pleuroscopy services using the latest flexible thoracoscopy equipment. This advanced technique provides better access, reduces the need for general anesthesia, and allows for early diagnosis of pleural diseases such as tuberculosis, malignancies, or infections.
Unlike traditional surgical methods, pleuroscopy with a flexible thoracoscope involves only local anesthesia and mild sedation. The procedure is performed through a small incision, making recovery faster and significantly lowering complication risks.
For patients requiring detailed pleural evaluation, flexible pleuroscopy is an ideal option. Trust Dr. Manoj Kumar Goel’s extensive experience and patient-focused approach for high-precision diagnosis and personalized pulmonary care.
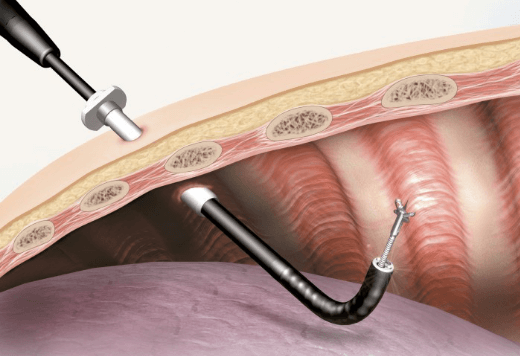
Intercostal Drainage Tube Placement (ICD) in Pleuroscopy
In cases where pleuroscopy identifies significant pleural effusion requiring drainage, an Intercostal Drainage Tube (ICD) may be placed. The site of intercostal tube placement is first localised clinicoradiologically or with the help of USG if required. Antiseptic dressing and draping are done, and local anaesthesia is given in and around the area of ICD placement. A small incision is made in the skin, followed by intercostal muscle separation to reach the pleural space. Through this small hole in the chest, the tube is guided and introduced into the pleural space. The ICD is connected to an appropriate drainage bag. The chest tube is kept in place for the duration it is required, which varies amongst patients.
Possible Risks and Complications of ICD
The incidence of major and minor complications associated with ICD are 1.9% and 5.5%, respectively. The complications include improper placement, tube dislodgement, coughing, shoulder pain, prolonged air leak, hemorrhage, subcutaneous emphysema, postoperative fever, empyema, wound infection, cardiac arrhythmias, reexpansion pulmonary edema, hypotension, seeding of chest wall in patients with mesothelioma, diaphragmatic tear, and injury to surrounding organs. There may be a need for thoracotomy and additional procedures. The mortality rate associated with ICD performed is 0.09%.
Post-Procedure Course for ICD
-
Postoperative oxygen supplementation may be required in some patients, particularly those with impaired lung function and those who have been sedated.
-
A chest radiograph is carried out post-procedure.
-
Patients should observe for pain, breathlessness, haemoptysis, surgical emphysema, and excessive coughing.